HYPEROIL
WOUND DEFINITION

The skin lesions, more or less deep, are breakdown areas with tissue loss and exposure of underlying tissues.
The term "external lesion" or "wound" denotes the destruction of morphological and functional continuity of the superficial skin layers and, in severe cases, deeper subcutaneous tissue.
The lesions are evaluated and categorized according to their width, depth and characteristics. Other considered factors are their development, causes (etiology) and pathophysiological context of the wound.
Superficial, minor lesions affect only the epidermis, the dermis and at most one part of the hypodermis; the deeper ones involve all the subcutaneous (fat) tissue up to the muscles, the periosteum, to bone exposure or support structures (tendons and cartilage); serious (chronic) ones are characterized by loss of substance in the skin and a low tendency to healing.
Depending on healing time, they can be divided into acute and chronic lesions. The acute ones heal through 3 different stages and reach the state of tissue repair by 8/10 weeks. Beyond this time the lesion becomes chronic, and if you do not act properly, the wound degrades in stages more and more serious.
Acute wounds that the health professional must deal with more frequently are surgical wounds.
Chronic tissue lesions involve the loss of substance affecting the epidermis, the dermis and the superficial and deep subcutaneous tissue; they tend to recur and difficultly heal spontaneously.
The chronic tissue lesions represent a significant risk factor for hospitalization, amputation, sepsis and mortality. From the point of view of the patient, lesions therapy is often painful and uncomfortable.

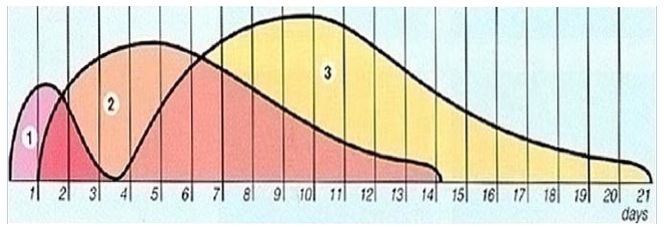
The wound healing process can be divided into different sequential, yet overlapping stages. When a lesion goes through these stages, the healing takes place. Unfortunately, chronic lesions due to systemic diseases or weakness and malnutrition conditions fail to progress through these stages and degenerate in progressively worse stages.
The diagram below shows the interaction between the three different stages of the wound healing process and its average time by primary intention (excluding a further period for remodeling).
Wound classification and their healing stages are important tools to research and choose the optimal topical therapy. Progetto Intesa – Medicazione Speciale This project was developed in collaboration with: A.I.S.Le.C. – Associazione Infermieristica per lo Studio delle Lesioni Cutanee (Nursing Association for the Study of Cutaneous Wounds) – Pavia Scientific coordination: Associazioni Titolari di Farmacia of Belluno, Bergamo, Bolzano, Lecco, Mantova, Pavia, Trento and Vicenza.03
There are different types of lesions categorization according to their characteristics. Some of them are used for all types of ulcers, while other only for certain types of lesions.
1) model based on "colour-coded" optical parameter, as proposed by Wound CareSociety.
Black wounds - Yellow wounds - Red wounds - Pink wounds
2) using a rating scale, as the one proposed by the National Pressure Ulcer Advisory Panel (NPUAP) divided into "four stages" according to the different layers concerned, and usually used to classify bedsores.
- Stage I, intact skin erythema, which does not disappear applying pressure; it classify a lesion that heralds the skin ulcer. On darkly pigmented skin, other symptoms can be a different color, loss of warmth, edema and swelling.
- Stage II, partial thickness skin loss involving epidermis, dermis or both. The lesion is superficial and clinically presents as an abrasion, a blister or a shallow crater.
- Stage III, full thickness skin loss involving damage to, or necrosis of, subcutaneous tissue that may extend down to, but not through, underlying fascia. Presents clinically as a deep crater with or without undermining.
- Stage IV, full thickness skin loss with extensive destruction, tissue necrosis, or damage to muscle, bone, or supporting structures (tendon or joint capsule). Undermining and sinus tracts may be associated with bedsores of stage IV.
In addition to this classification, which is the most widely used, there are other models:
- SHEA scale (4 stages)
- Agency for Health care Policy (4 stages)
- SESSING scale (7 stages)
- American Geriatric Society (5 stages)
- EPUAP - European Pressure Ulcer Advisory Panel - Guidelines (4 stages)
3) through specific classifications for foot lesions in diabetic patients, such as that proposed by Wagner.
- Grade 0: no ulcer, but risk of lesion for the presence of neuropathic and vascular complications;
- Grade 1: ulcer limited to the dermis (skin and subcutaneous tissue);
- Grade 2: Deep ulcer extending through tendon and joint capsules, no infection;
- Grade 3: Deep ulcer extending through bone, with or without osteitis or osteomyelitis;
- Grade 4: Localized gangrene (forefoot or heel);
- Grade 5: Gangrene of the foot.
4) The University of Texas has recently adopted a classification that can be considered, quite rightly, more complete and articulated.
The lesions are evaluated depending on severity (in grade) and pathogenic moment (in depth), allowing a satisfactory clinical definition.

5) There is also a STATUS classification of the lesion:
The ulcer, once formed, can be present in one or more of the following statuses:
- Necrotic
- Colliquative (the colliquation is a degenerative process that involves the fluidization of a tissue; the degenerative process of a tissue accompanied by liquefaction of necrotic material)
- Infected
- Fibrinous
- Fibrin-membranous
- Cleansed (that do not include foreign bodies or metabolic debris)
- With granulation tissue
The lesion can also be:
- poorly exudative (a fluid resulting from exudation composed by blood plasma and white blood cell, erythrocytes, etc. that has escaped from blood vessels as a result of a wound. This fluid deposits in tissues or on tissue surfaces inducing BIOFILM formation.exudate
: fluid produced by the lesion, consisting of serum, leukocytes and devitalized material. Volume decreases as tissue repair progresses. The exudate may have bactericidal properties and contain nutritional factors. It can also be infected)
- exudative
- heavy exudative
and can be:
- undermined and/or with tunnels and/or fistulas (Fistula: an abnormal communication tract between an inner tissue and the skin)
This need to classify and evaluate is just the logical and practical result from difficulties arising from treating chronic lesions.
The lack of a unique product that could assist in the treatment at any time of the lesion, has created the need to choose a common evaluation system, in order to indicate the various dressings to be used according to the condition of the lesion.
For this reason and for the complexity of the lesions, the models have multiplied. If it was not necessary to treat differently each stage/grade/state/phase of a lesion, it would not make sense to create different classifications. That's why it is a real revolution having a single product able to assist in the treatment of any lesion at all times.
Send us a message

Via Manuzio 15
41037 Mirandola (MO) | Italy


8:30AM - 12:30PM
2:00PM - 5:30PM
